Feeling like you have not fully emptied your bladder after urinating is more than just uncomfortable. Over time, urine that stays in the bladder can cause recurrent infections, damage the kidneys, and significantly affect daily life. Bladder not emptying completely treatment is available for all underlying causes, and outcomes are best when the condition is identified and addressed early.
This guide explains what causes incomplete bladder emptying, how it is diagnosed, and what treatment for incomplete bladder emptying is available for both men and women.
What is Incomplete Bladder Emptying?
Incomplete bladder emptying means the bladder does not fully empty when you urinate. Some urine remains inside, called post-void residual (PVR) urine. A post-void residual of less than 50 ml is generally considered normal, although interpretation depends on age and clinical context. A consistently elevated PVR, particularly above 100 to 150 ml, is considered clinically significant and warrants investigation.
The condition exists in two forms.
Acute urinary retention is a sudden, complete inability to urinate. It is painful and constitutes a medical emergency requiring immediate treatment.
Chronic urinary retention develops gradually. The bladder does not empty fully over time, often without severe pain. Many people with chronic retention are unaware of it until they develop a urinary tract infection, feel persistent urge, or have it detected on an ultrasound scan. Chronic urinary retention treatment focuses on identifying the underlying cause and restoring normal bladder function before complications develop.
Symptoms of Incomplete Bladder Emptying
Symptoms vary depending on whether the retention is acute or chronic.
Common symptoms include:
- A persistent feeling of needing to urinate even after just going to the toilet
- Frequent urination, especially at night
- A weak, slow, or interrupted urine stream
- Straining to start urination
- Dribbling at the end of urination
- Recurrent urinary tract infections
- Lower abdominal discomfort or a sense of pressure
In acute retention, the inability to pass urine at all despite a strong urge and significant lower abdominal pain are the defining features. This needs emergency evaluation without delay.
What Causes Incomplete Bladder Emptying?
Incomplete bladder emptying results from one of two main problems: an obstruction that blocks urine from flowing out, or a bladder muscle that is too weak to contract fully.
Obstructive Causes
Benign prostatic hyperplasia (BPH) is the most common cause in men over 50. As the prostate enlarges, it compresses the urethra and restricts urine flow. This is the leading cause of incomplete bladder emptying in men.
Urethral stricture is a narrowing of the urethra due to scar tissue from previous infection, injury, or surgery. It reduces the channel through which urine can pass.
Bladder stones can occasionally shift to block the bladder outlet, causing sudden obstruction.
Pelvic organ prolapse in women, where the bladder, uterus, or rectum descend into the vaginal canal, can kink or compress the urethra and obstruct normal urine outflow.
Constipation causes the full bowel to press against the bladder and urethra, particularly in women and older adults, contributing to incomplete emptying.
Neurological Causes
Diabetic neuropathy affects the nerves controlling bladder contraction. People with long-standing or poorly controlled diabetes are at high risk of developing an underactive bladder that cannot empty fully.
Spinal cord injury or disease can disrupt the nerve signals between the brain and the bladder, causing either overactivity or underactivity of the detrusor muscle.
Multiple sclerosis, Parkinson’s disease, and stroke all affect neurological control of the bladder and can result in incomplete emptying or, in some cases, complete retention.
Bladder Muscle Weakness
The detrusor muscle, which contracts to push urine out, can become weak over time. This happens with age, after long periods of chronic overdistension of the bladder, as a side effect of certain medications, or as a result of the neurological conditions listed above.
Certain medications are also known to reduce bladder contractility, including some antihistamines, antidepressants, antipsychotics, and medications with anticholinergic effects. If you have recently started a new medication and noticed bladder symptoms, inform your doctor.
How is Incomplete Bladder Emptying Diagnosed?
Accurate diagnosis is essential before any treatment is started. The cause determines the treatment entirely.
Post-void residual (PVR) measurement is the most important first test. An ultrasound scan is performed after you urinate to measure how much urine remains in the bladder. It is painless, takes only a few minutes, and gives an immediate result.
Uroflowmetry measures the speed and volume of your urine flow. A weak or interrupted flow pattern helps identify whether obstruction or weak bladder muscle is contributing.
Urodynamic studies are more detailed tests that assess bladder pressure, muscle activity, and bladder capacity during filling and emptying. They are particularly useful when the cause is unclear or neurological in origin.
Ultrasound of the kidneys and bladder assesses whether chronic retention has caused the kidneys to enlarge due to back pressure (hydronephrosis).
PSA blood test and prostate assessment in men helps evaluate the prostate’s size and role in obstruction.
Cystoscopy allows direct visualisation of the urethra and bladder interior to identify strictures, stones, or tumours contributing to obstruction.
Incomplete Bladder Emptying Treatment Options
Treatment depends entirely on the cause, the severity of residual urine, and the presence or absence of complications such as infections or kidney involvement.
1. Treating the Underlying Cause
The most effective long-term approach is addressing what is causing the incomplete emptying directly.
For BPH, treatment ranges from alpha-blocker medications to surgical removal of excess prostate tissue. For urethral stricture, dilatation or urethroplasty restores the channel. For pelvic organ prolapse, surgical repair removes the obstruction. For diabetic neuropathy, better blood sugar control slows further nerve damage.
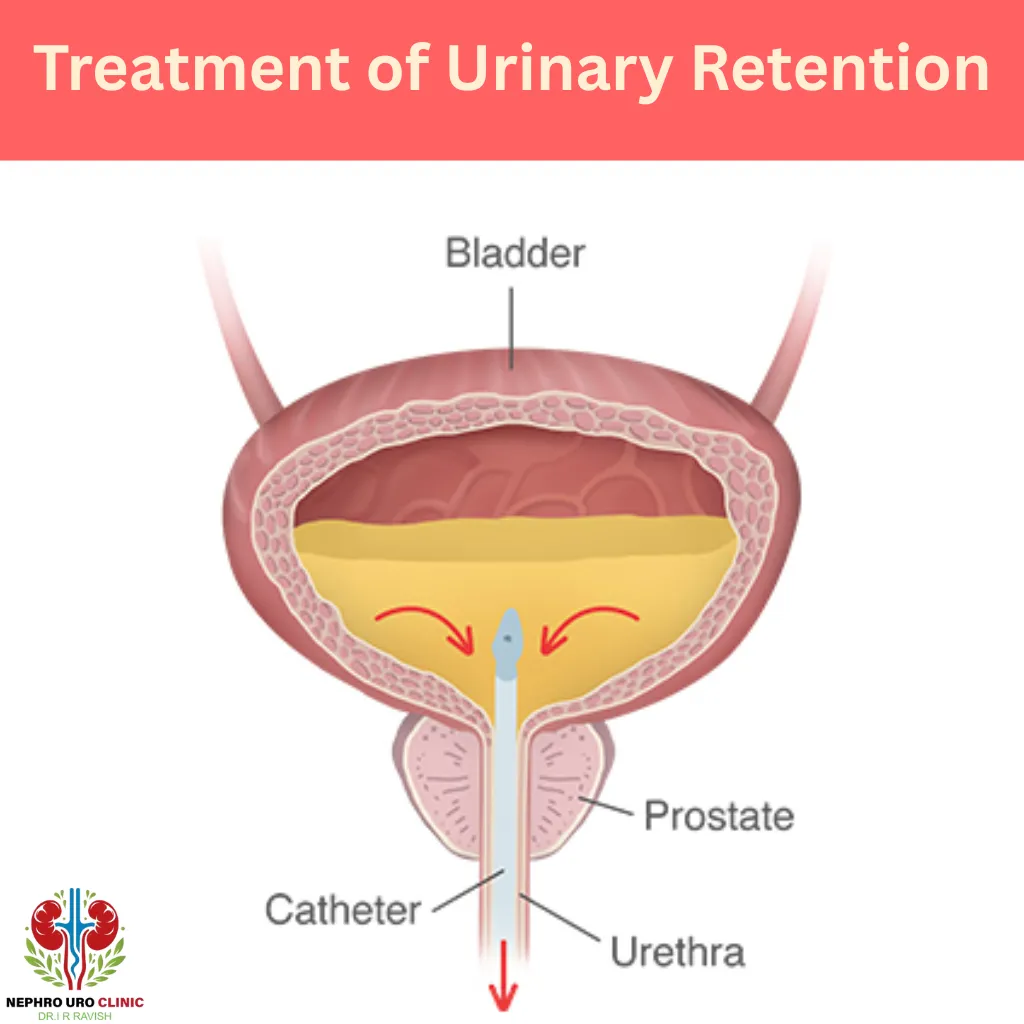
2. Bladder Drainage: Catheterisation
When retention is significant, the bladder needs to be drained to relieve pressure and prevent kidney damage while the underlying cause is being assessed and treated.
Urethral catheterisation involves inserting a thin flexible tube through the urethra into the bladder to drain the urine. In acute retention, this is done immediately as an emergency procedure. It provides instant relief of pain and pressure.
Intermittent self-catheterisation (ISC) is a technique where the patient inserts and removes a small catheter several times a day to empty the bladder completely. It is recommended for chronic retention caused by neurological conditions or a weak bladder muscle. With proper training, most patients manage ISC independently and find it gives them back a sense of control over their bladder function.
Indwelling catheter (urethral or suprapubic) is used for patients who cannot perform ISC or who have severe, irreversible retention. A suprapubic catheter is inserted through a small opening in the lower abdomen directly into the bladder, which many patients find more comfortable for long-term use than a urethral catheter. Indwelling catheters require regular care and monitoring to minimise infection risk.
3. Medications
Several medications are used depending on the underlying cause.
Alpha-blockers such as tamsulosin and alfuzosin relax the smooth muscle of the prostate and bladder neck, improving urine flow in men with BPH. They are usually the first medication tried and work relatively quickly.
5-alpha reductase inhibitors such as finasteride and dutasteride reduce prostate size over several months. They are used for men with significantly enlarged prostates and are often combined with alpha-blockers for better effect.
Antibiotics are prescribed when urinary tract infection is present alongside retention. Treating the infection reduces bladder irritability and can improve emptying.
4. Minimally Invasive Procedures
Urethral dilatation involves gently widening a narrowed urethra using progressively sized instruments. It improves urine flow and may need to be repeated if the stricture recurs.
Urethral stents are small tubes placed inside the urethra to keep it open in cases of recurrent stricture. They are effective but require monitoring for potential complications such as migration or infection.
UroLift is a minimally invasive procedure for men with BPH where small implants hold the enlarged prostate lobes apart, widening the urethral channel without removing tissue. It is done under light sedation, preserves sexual function, and has a short recovery time.
5. Surgery
Surgery is considered when conservative treatments have not provided adequate relief or when the underlying cause specifically requires surgical correction.
Transurethral resection of the prostate (TURP) removes excess prostate tissue obstructing the urethra and is a well-established procedure for significant BPH. It provides durable long-term improvement in bladder emptying.
HoLEP (Holmium Laser Enucleation of the Prostate) is a modern laser-based alternative to TURP that is particularly effective for large prostates. It has a strong safety profile and excellent long-term outcomes.
Urethroplasty surgically reconstructs a strictured urethra using tissue grafts and offers the best long-term cure rates for urethral stricture disease compared to dilatation alone.
Pelvic floor repair surgery in women corrects prolapsed pelvic organs that are compressing the urethra.
6. Pelvic Floor Rehabilitation
In women with pelvic floor dysfunction contributing to incomplete emptying, physiotherapy targeting the pelvic floor muscles can improve bladder emptying. A specialised pelvic floor physiotherapist provides guided exercises tailored to whether the muscles need strengthening or relaxation.
7. Double Voiding
Double voiding is a simple behavioural technique that can help some patients empty their bladder more completely. After urinating, the patient waits one to two minutes and then tries to urinate again. This gives the bladder a chance to contract a second time and expel residual urine. It is particularly useful for people with mild incomplete emptying and no structural obstruction.
Complications of Untreated Incomplete Bladder Emptying
Leaving significant incomplete bladder emptying untreated over time can lead to:
- Recurrent urinary tract infections caused by bacteria multiplying in the stagnant residual urine. Repeated infections can scar the bladder lining over time.
- Bladder stones forming from minerals that crystallise in retained urine.
- Bladder damage from chronic overdistension, where the bladder walls stretch and lose their ability to contract effectively.
- Kidney damage and hydronephrosis if back pressure from a full bladder causes the ureters and kidneys to swell. In severe cases, this can progress to chronic kidney disease.
- Acute on chronic retention where a person with existing chronic retention suddenly becomes unable to urinate at all, requiring emergency catheterisation.
Early treatment prevents these complications and protects long-term kidney and bladder function.
When to See a Urologist
See a urologist promptly if you experience any of the following:
- Complete inability to urinate, which is a medical emergency
- Recurrent urinary tract infections (two or more in six months)
- A persistent weak stream, straining, or dribbling after urination
- Frequent waking at night to urinate combined with a sense of incomplete emptying
- Blood in the urine
- Lower back or flank pain alongside urinary symptoms
- Any urinary symptoms in the context of diabetes, neurological disease, or a history of pelvic surgery
At Nephro Uro Clinic in Bengaluru, Dr. I. R. Ravish evaluates incomplete bladder emptying with a thorough assessment including PVR measurement, uroflowmetry, and targeted imaging. A clear diagnosis is established before any treatment is recommended, and the management plan is tailored to each patient’s specific cause, symptoms, and overall health.
Can Incomplete Bladder Emptying Be Cured?
Many cases can be significantly improved or completely resolved once the underlying cause is treated.
When the cause is obstructive, such as BPH or urethral stricture, surgical or procedural treatment reliably restores normal bladder emptying in the majority of patients. When pelvic organ prolapse is responsible, surgical repair typically resolves the problem.
When the cause is neurological, such as diabetic neuropathy or spinal cord disease, complete cure is less predictable. However, symptoms can almost always be effectively managed to prevent complications and maintain quality of life. Intermittent self-catheterisation and targeted medication allow most patients to live well despite an underlying neurological condition.
When bladder muscle weakness is the cause, outcomes depend on severity. Early intervention before the muscle becomes severely damaged gives the best results, which is another reason to seek evaluation promptly rather than waiting.
In summary, the likelihood of cure or significant improvement is high when the condition is caught and treated before significant bladder or kidney damage has occurred.
Conclusion
Incomplete bladder emptying is a common but underreported condition that affects men and women of all ages. The causes range from an enlarged prostate to nerve damage to pelvic organ prolapse, and treatment depends entirely on identifying which of these is responsible.
The important thing to understand is that this condition is treatable. Whether the solution is a simple medication, a minimally invasive procedure, or a short course of physiotherapy, most people see significant improvement with the right care.
Do not ignore persistent bladder symptoms or assume they are a normal part of aging. Early evaluation leads to simpler treatment and prevents the long-term complications that arise when incomplete emptying goes unaddressed for years.
Read also How to Prevent Urinary Tract Infections.